


Are Vaccines Lowering Risk of Death and Hospitalizations or Not?
If we don't know for sure, well, that's a problem.


This is so important to get correct. Many decisions are based on this one question. And to this day it’s still not 100% clear (to an objective eye) if the answer we are given by authorities is in fact, correct.
We will NOT discuss transmission in this post, it’s clear since omicron arrived the vaccines are useless in that regard, though some still peddle it (still 30-60% transmission reduction!”) with no real evidence. In my own lived experience I knew in the ~20 months before omicron 5 people that tested positive for Sars2. After omicron that number is now 25 and about all are boosted. Enough, it’s a transmission failure. All were fine after a few days BTW.
The Official Line
Vaccines reduce deaths and hospitalizations by 90-95%. On a bad day you may get a number expressed as X amount. We have seen 100X, 94X, 54X, 34X, 10X just to list a few. Quite the range for such an effect!
A few examples:
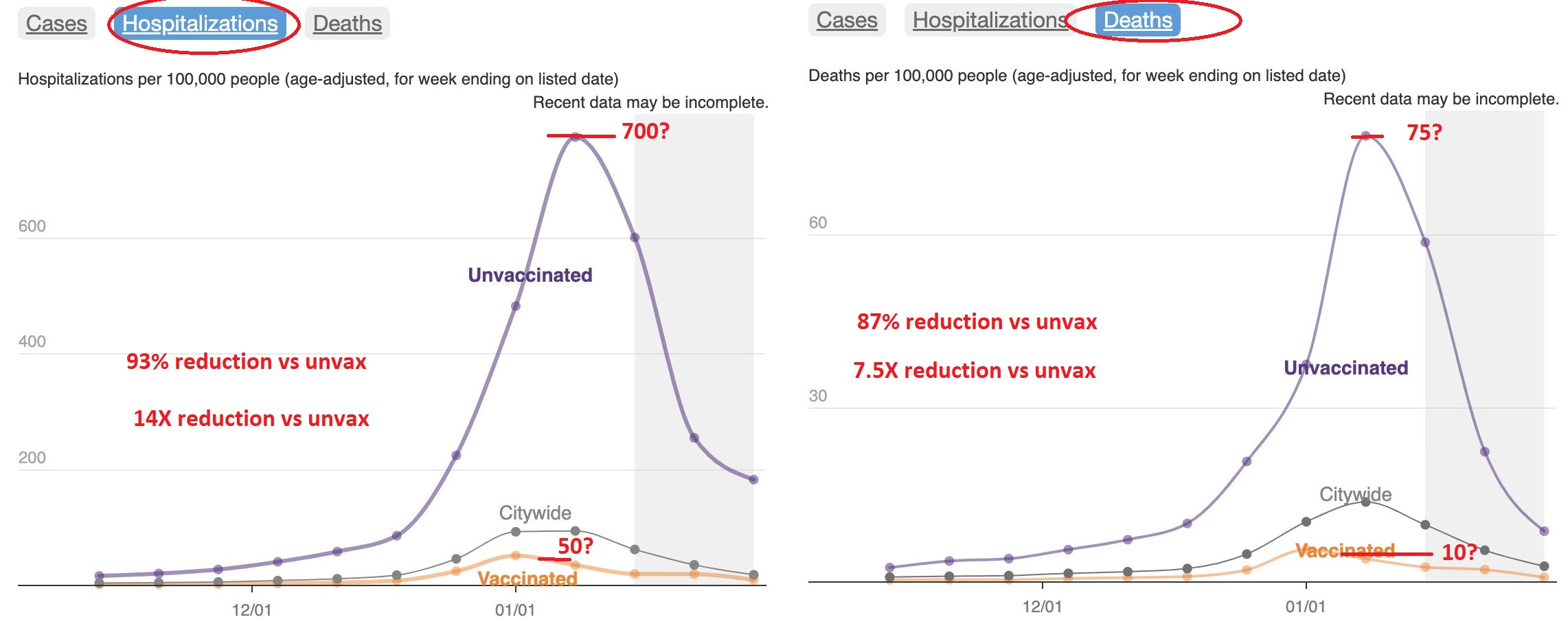
The famous (or infamous) NYC data sets pushed non-stop a few weeks ago:
(My best guesses on numbers, the scales are terrible on charts)
Eric Topol was out February 18th with this set:
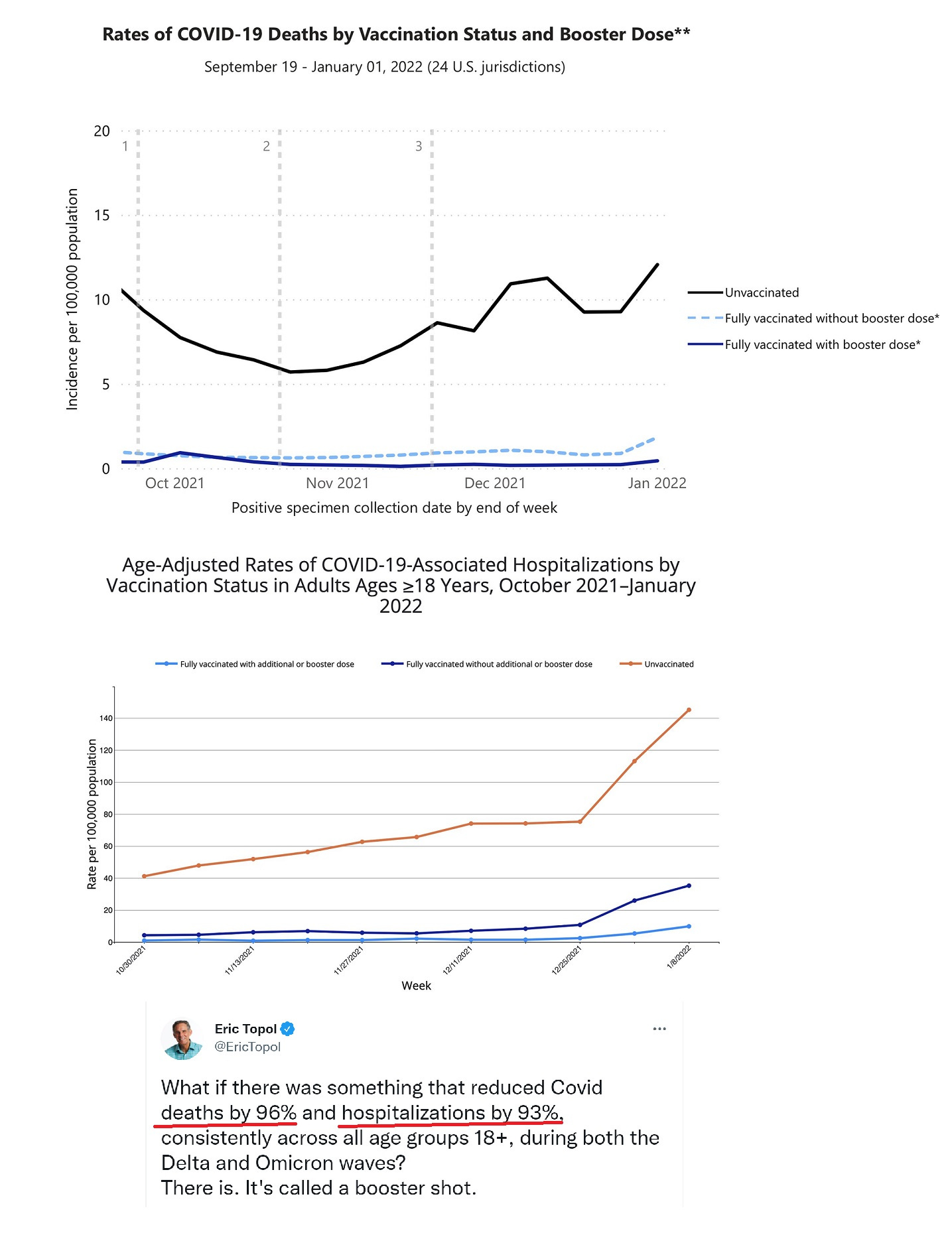
This one is booster centric, bust just plain vaccinated is not far from boosted on these charts, so we can use about the same numbers of 96% and 93% that he does.
So it's all there, black and white, clear as crystal.
Looking Under the Hood
Some have known me for a LONG time and for those that do, they know I was the biggest cheerleader for vaccines that there was. I followed the clinical trials and all the data that was leaked running up to the final EUA approval.
I was astounded by the ability to both stop transmission and seemingly end adverse outcomes. We had never in all of history had an effective coronavirus vaccine and yet it seemed we now did. I was proud of being a scientist and all we can do when given the chance.
As a “essential worker” in bio-science I was able to get a vaccine as early as January 2021. I waited. Early on the doses were limited and I wanted the most at risk (over age 65, health issues) to have full access. I would not steal a dose, I felt it morally incorrect to do so.
And the seasonal winter wave died out, and vaccine roll out went along.
Then a lot of my friends started having reactions to the vaccines. A LOT of them. Nothing insane, but certainly not usual post vax sorts of things.
I was vaccinated with J&J in May 2021, even given my fears due to severe blood clot risks in males in my family (both Father and Brother died of transient clots at ages 50 and 36 respectively) and after a warning the J&J has that possible rare side effect. Took my shot. For society. And to keep my job. To be left the F alone.
Then Pfizer published a supplemental follow up report, and I saw they stashed a large number of Sars2 infected trial subjects after the 1st dose of Pfizer into the unvaccinated cohorts, wildly distorting the end result. These infections would have invalidated the entire trial, and approval never given. Little did I know, it mattered little.
Anyways, since then I always look at data when we can get it as well as look to other countries for accurate reports. The US purposely massages and adjusts data sets or just does not report them at all. Why?
Even today the NY Times had this:

Now Apoorva Manavilli is the CDC’s chosen info publisher, so it’s weird she ran this. Why now?
Some snippets:
When the C.D.C. published the first significant data on the effectiveness of boosters in adults younger than 65 two weeks ago, it left out the numbers for a huge portion of that population: 18- to 49-year-olds, the group least likely to benefit from extra shots, because the first two doses already left them well-protected.
As we know, boosters for all were approved some time ago without this critical population set data. It was available, so why was it withheld? Why indeed. A pattern emerges:
Kristen Nordlund, a spokeswoman for the C.D.C., said the agency has been slow to release the different streams of data “because basically, at the end of the day, it’s not yet ready for prime time.” She said the agency’s “priority when gathering any data is to ensure that it’s accurate and actionable.”
Another reason is fear that the information might be misinterpreted, Ms. Nordlund said.
The plebs cannot see the unadjusted data, or they may get a certain idea. Got it.
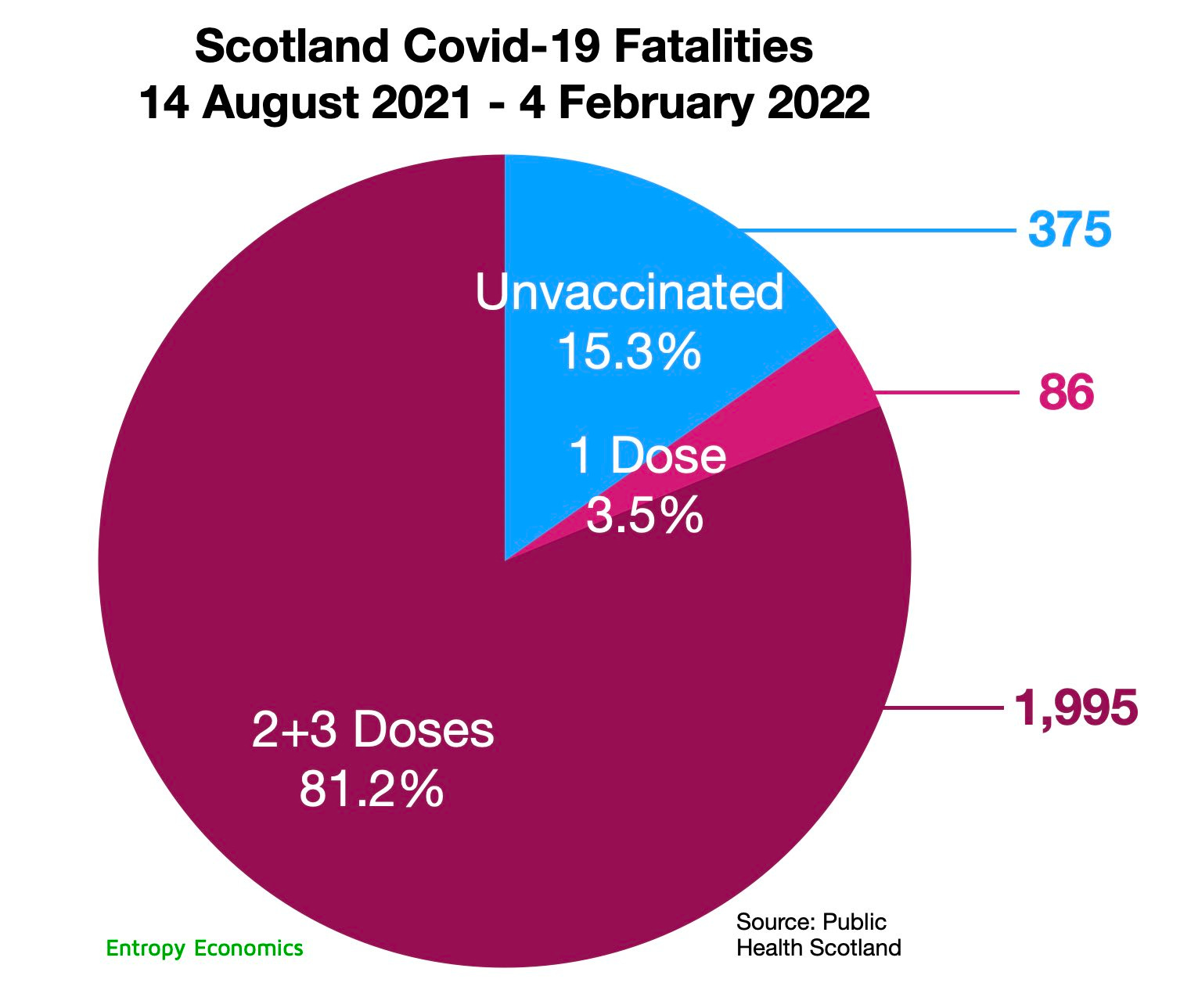
Concern about the misinterpretation of hospitalization data broken down by vaccination status is not unique to the C.D.C. On Thursday, public health officials in Scotland said they would stop releasing data on Covid hospitalizations and deaths by vaccination status because of similar fears that the figures would be misrepresented by anti-vaccine groups.
Now we are getting to the crux of it.
Scotland, huh?
Like this data?:
Recap here:



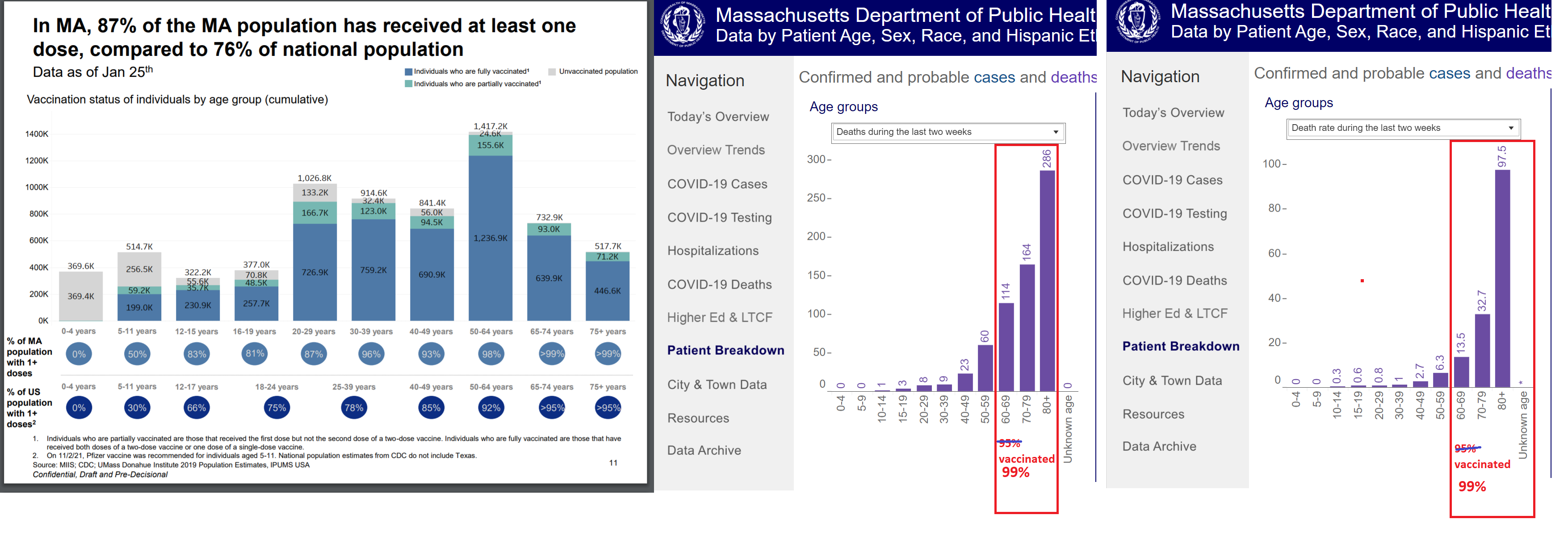
Massachusetts publishes good data and again, it’s a far different story than we are told:
The UK data:
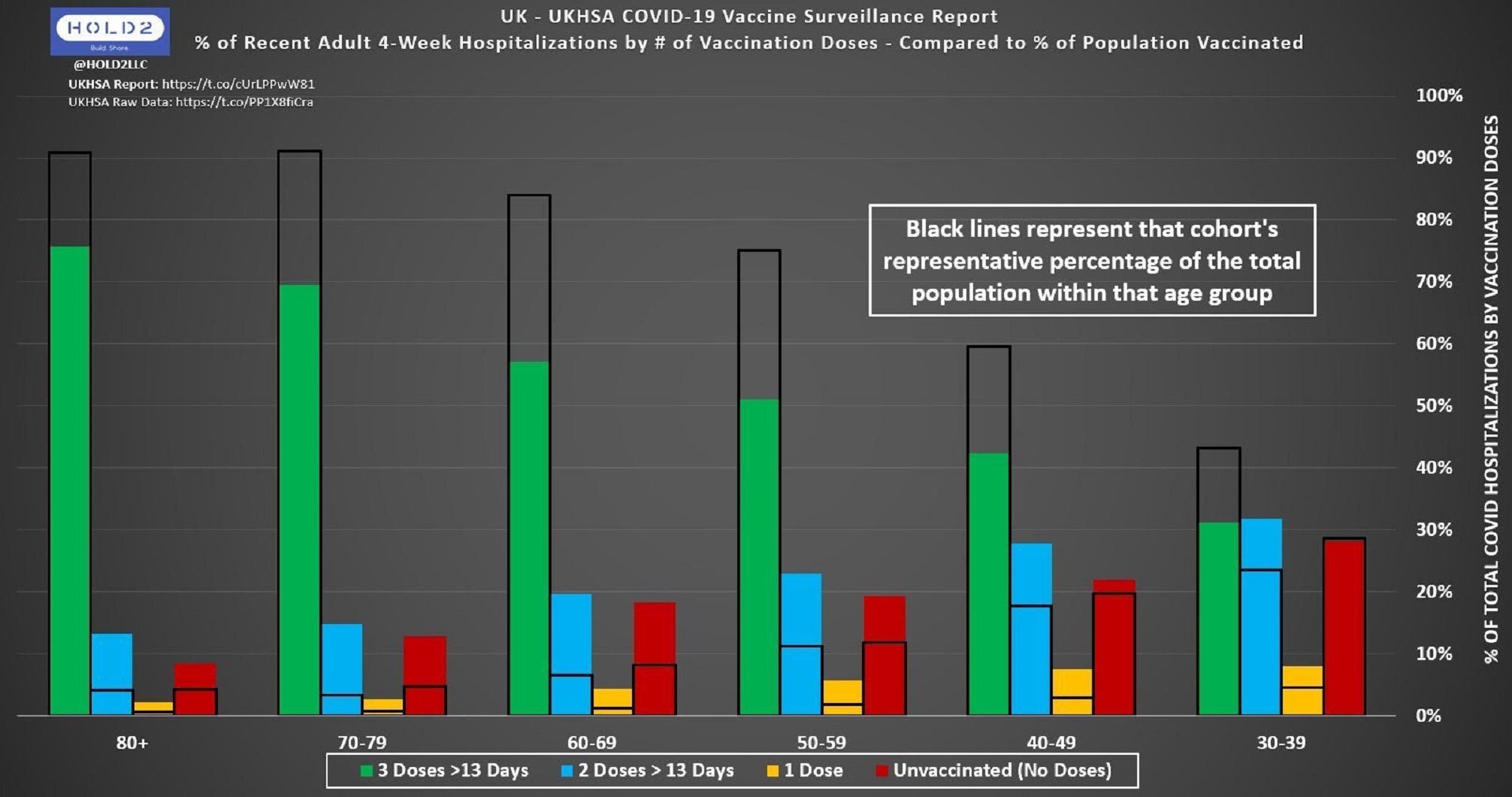
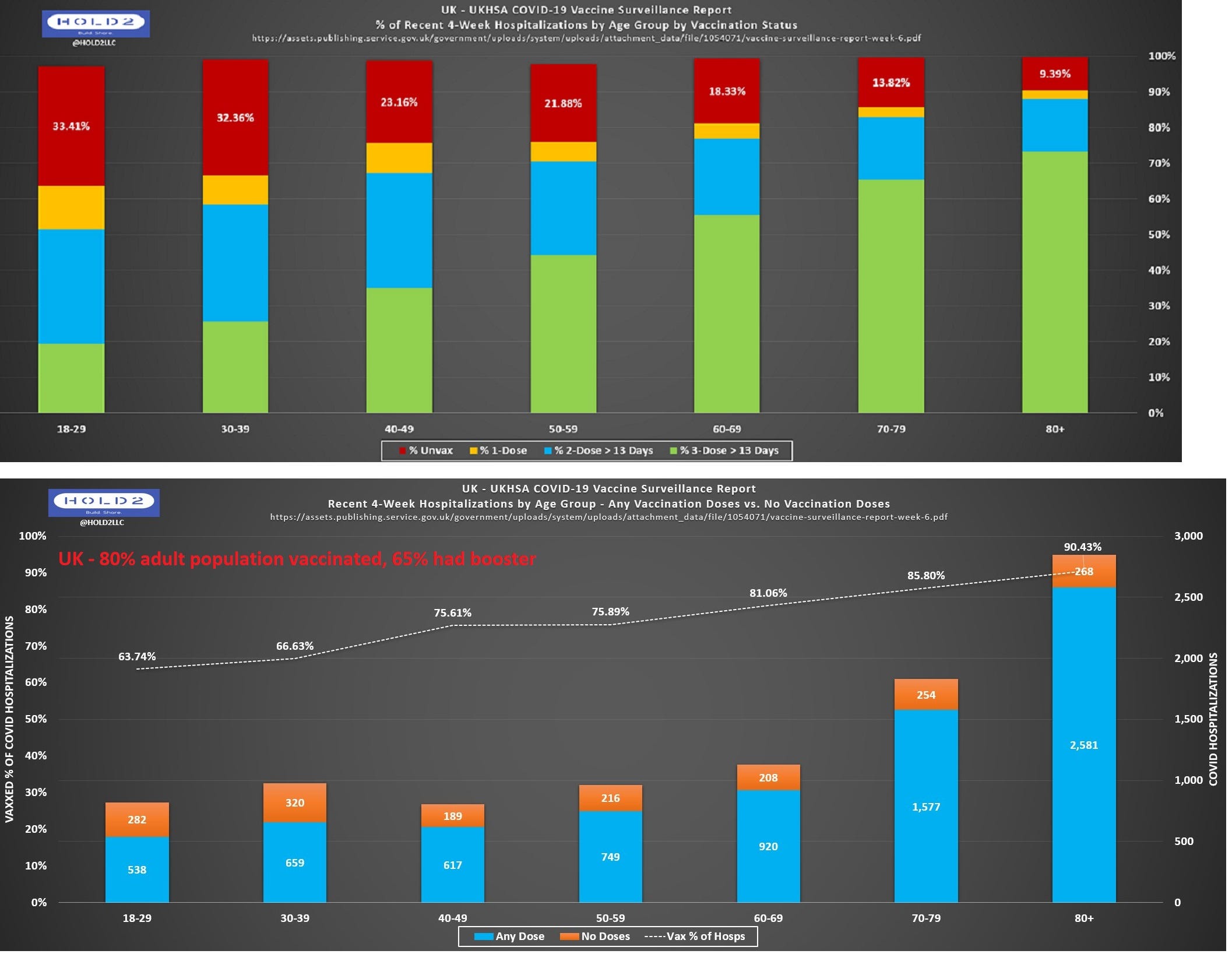
You can just keep scrolling on Hold2LLC’s runs here:



Confronted with this type of granular data, the best move is to consider it and think. Doctors etc instead lash out, as if their very religion has been assaulted. Sam here says only 10% of hospitalizations are vaccinated and only 1% of deaths are vaccinated in his hospital, better than even the CDC says!


He provides no data to back this up, for what it’s worth.
Ok, so where are we?
The “Age Adjusted Data” is Culprit #1
In my opinion, the major problem here is an effort to somehow remove the older aged people from the vaccination counts, they are “age adjusted” away.
From the Massachusetts data we see the 95% plus vaccinated over age 60 group is 80-90% of all deaths. There are simply not enough unvaccinated in that age group to make this work. So my guess is they are weighted in a way to make them irrelevant. Which takes advantage of the fact that people under age 50 rarely die of covid anyway, vaccine or not.
Say a model gives:
Age 18-45 FOUR (4) points
Age 46-55 TWO (2) points
Age 56-65 One (1) point
Ages 66 and older 0.4 points
Now we run the numbers for vaccinated vs unvaccinated bases on their population %’s again. And….wow it comes out about on spot for deaths and hospitalizations as shown by NYC and CDC charts. Work not shown as I am still tinkering.
All this can be solved tomorrow: The CDC and NYC and any place that uses “adjusted” data should show the model used for review. Easy. Could not be easier.
Vaccine Records Matching is Culprit #2
Again, Hold2LLC has covered this in detail, and it’s beyond me to redo all that here.
Easy visual:

There are many other issues but they all boil down to one over arching problem, which I will lay out next.
What if the Vaccines Did Not Work Well?
This is a THOUGHT EXPERIMENT for now and not my opinion or stance. Just a thought, go with it.
Say the vaccine didn’t lower hospital use or deaths more than 10% or even not at all, how would you know?
Really, how would you know? I would like answers, ideas.
Age adjusted data sets by the CDC would still show an amazing effect of vaccines as they already do. They would look no different, the adjustments would just change.
We are told daily “older folks with several comorbidities sadly often still die of covid, a vaccine cannot save them all.” It would be the same if they did nothing at all.
Hospital usage rates have been stable since May 2020, so how would you know the vaccine is lowering usage rates? Who reports those numbers?
What government on Earth would say “hey, we spent a gazzilion dollars on the vax, threatened you with losing your job, made you wear a mask, and excluded you from society over this vax, but our bad!!! No biggie, let’s just move on. All in this together right?”. None could or would.
Ultimately if the vaccine worked as well as reported there would be no need to adjust any data, or not report data collected, nor launch crusades against misinformation. It would just be obvious to all with no massaging. Tell me clarithromycin does not work against bronchitis and I KNOW FOR A FACT that’s bullshit. No need to age adjust the data, nor censor people that say it’s useless, I KNOW it works. I cannot say that for the vaccines.
As an ending thought, if they work so amazing, why a 3rd dose? And a planned 4th dose? And an omicron specific dose X 3? What’s up with that?
Hints are Everywhere
All I can say is get ready, this needs more attention.
Say 50% of the US had covid before mass vaccine rollout. How can you tell if vaccines are working? We have both the immortality issue (removal of susceptible people {death} from population causes bias for remaining set) and the fact that vaccination after infection provides no additional gains? If 50% of the population is already functionally immune, how can we know the vaccine works? It’s a a tough one.





Ooooof.
Cultural Corner
“The Goods: Live Hard, Sell Hard” (2009)
I have yet to see this but now I want to!
Have a good night.